Small animal veterinary case study – Freuchie the cavalier king charles spaniel
Case provided by Yvonne McGrotty BVMS CertSAM DipECVIM-CA MRCVS
European Specialist in Veterinary Internal Medicine
RCVS Specialist in Veterinary Internal Medicine

Freuchie was presented with a history of lethargy and collapse.
Physical examination
On clinical examination Freuchie was dull but responsive and in poor body condition with a body weight of 7.6kg. Mucous membranes were pale with prolonged CRT. A heart murmur was audible loudest over the tricuspid valve. His coat was dry and scurfy with scaling and crusts. The femoral and metatarsal pulses were absent in the right hind limb although the foot still felt reasonably warm. The left anal sac was thickened on rectal examination. Freuchie could walk but gait was abnormal and he was weak in the hindquarters.
Clinical pathology
Haematology revealed a mild regenerative anaemia (too mild to account for pallor) and a significant neutrophilia with a left shift consistent with active infection or inflammation.
Eosinophilia was also present. Thrombocytopenia was present but macrothrombocytes were present along with anisothrombia so this may just be a breed specific change although counts were somewhat lower than usually expected in this breed. An ACTH stimulation test was within acceptable range which is not supportive of hyperadrenocorticism but neither does this exclude it.
UPCR was increased at 1.7. TT4 was measured 3 days after last dose of thyroxine was administered and was well within reference range which was surprising. Urine culture was negative. Angiodetect was also negative. Blood culture results are pending.
Follow-up PCV after fluid therapy was 25%.
Diagnostic imaging
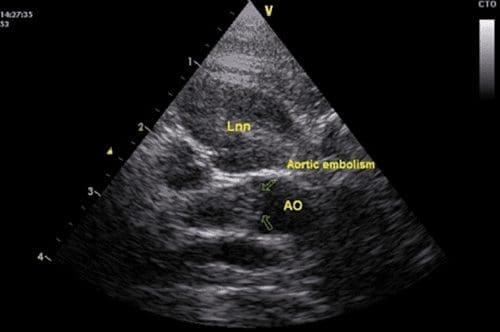
An abdominal ultrasound confirmed the presence of bilateral iliac lymph node enlargement (Approx 1.09 x 1.49cm). FNAs were obtained;. The left and right iliac lymph nodes contained a mixed lymphoid population with frequent plasma cells, eosinophils and macrophages consistent with a reactive change. The caudal pole of the spleen showed some irregularities. The parenchyma here appeared moth-eaten and reticular. Aspirates were obtained and results were consistent with extramedullary haematopoiesis and evidence of inflammation
A left sided adrenal mass was identified with no obvious signs of invasion into the major vessels. The maximum width was 0.9cm and the adrenal had lost its peanut shape. The right adrenal was unremarkable.
An aortic embolism was identified at the trifurcation and was occluding the majority of the blood flow to the right iliac artery. Both kidneys had evidence of mild pyelectasia possibly as a result of fluid therapy. The liver was enlarged and hyperechoic which may have been related to endocrine disease. The stomach and intestinal tract were unremarkable. The urinary bladder was small.


Diagnoses
- Thromboembolic disease with occlusion of right iliac artery
- Left adrenal mass
- Iliac lymph node enlargement
- Splenic changes
- Hypertension and proteinuria
- Tricuspid valve disease
- Anal sac disease
- Hypothyroidism