Small animal veterinary case study – Mika the dachshund
Small animal veterinary case study provided by Yvonne McGrotty BVMS CertSAM DipECVIM-CA MRCVS
European Specialist in Veterinary Internal Medicine
RCVS Specialist in Veterinary Internal Medicine

History of Small animal veterinary case study
Mika was presented with a 3 month history of dribbling urine unconsciously while asleep and excessive licking of the preputial region. More recently he had been straining to urinate and only passing small volumes of urine or interrupted streams of urine. The individual experienced an increase in the frequency of urination. Additionally, their appetite reduced, although there was no history of vomiting or diarrhea.Thirst was normal. Also Mika had been whining and yelping recently. Urinalysis revealed concentrated urine with an inactive sediment.Therefore, the medical team administered Propalin syrup, which reduced the frequency of the dribbling, and antibiotics. The owner also noted some improvement as a result of the treatment.
Physical Examination:
On clinical examination Mika was very bright and alert and in good body condition at 6.4kg. Mucous membranes were pink and moist and pulse quality was good. Thoracic auscultation was unremarkable. Mika showed signs of pain on palpation of the caudal abdomen over the bladder. The bladder felt fairly small. There was no evidence of any lesions on the prepuce or penis and no penile discharge.
Clinical Pathology:
Urine collected by cystocentesis contained 4+ blood. Crystals were not identified on a sediment exam. Biochemistry and electrolytes were unremarkable.
We have submitted the urine for further culture, and we are currently awaiting the results.
Diagnostic Imaging:
After sedating the patient, the medical team conducted an abdominal ultrasound. There was no free fluid and no enlarged LNs. The liver and spleen were unremarkable. The gastrointestinal tract was unremarkable. And both kidneys were unremarkable with good peripheral blood flow and no evidence of pelvic dilation.
The moderately distended bladder contained a large volume of hyperechoic corpuscular debris. Furthermore, the bladder wall exhibited thickening and irregularity both cranioventrally and towards the trigone, as shown in Figure 1.
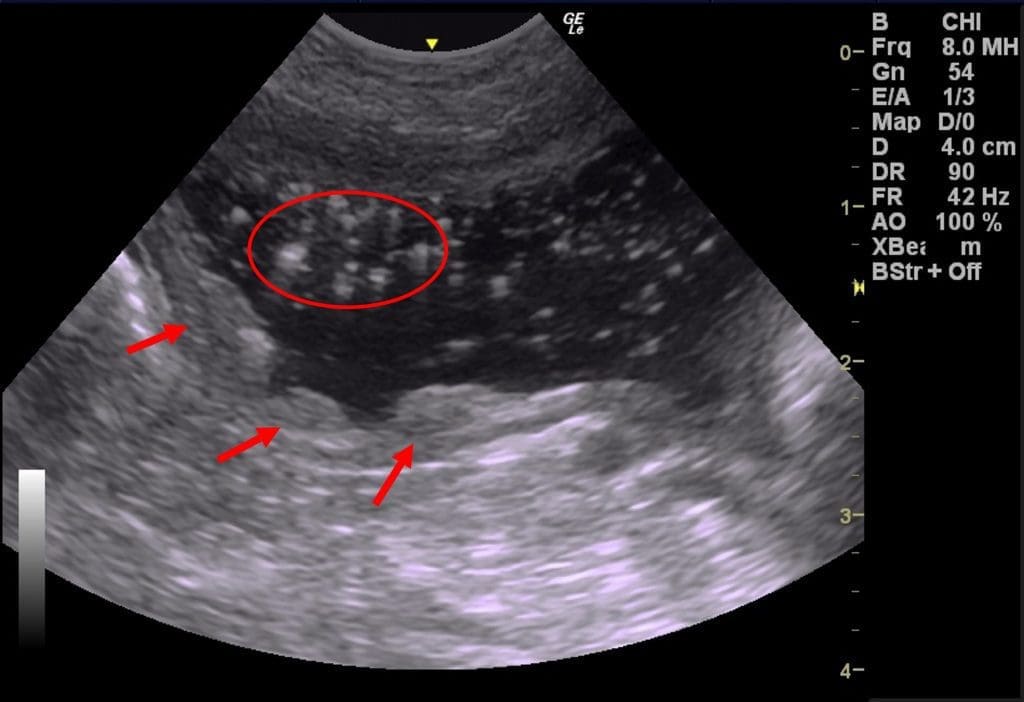
Figure 1.
In this sagittal plane image of the bladder, we can observe hyperechoic debris suspended within the urine (indicated by the red circle), and we also notice thickening and irregularity in the cranioventral bladder wall (highlighted by the red arrows).
The medical team performed radiographs of the caudal abdomen.There is a non-union fracture of the left acetabulum with lateral displacement of the iliac fracture segment. Moderate remodelling changes of the left femoral head are noted. There are also chronic non-union fractures of the left and right pubic and ischial bones.
Under sedation we attempted to catheterise the urethra. We noted an obstruction to the passage of a small gauge catheter approximately 4 cm inside the urethra. After passing this region, we advanced the catheter to a distance of 18 cm, but were unable to progress it further.
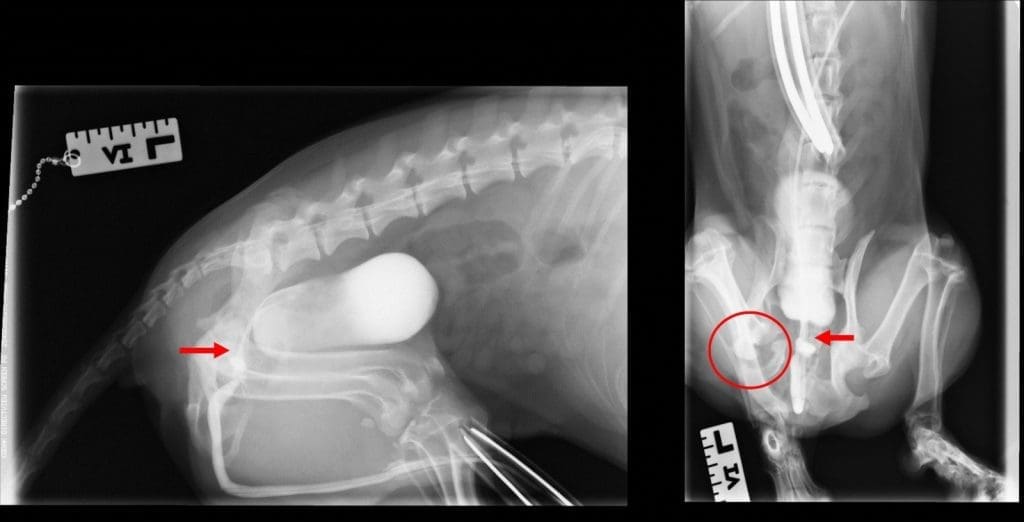
The medical staff performed enemas and administered a general anesthetic. A retrograde urethrogram was then performed. There is persistent focal narrowing of the prostatic urethra with focal mild dilation on either side of the narrowed region (Figure 2). No other significant urethral abnormalities are seen. There is a mild amount of reflux of contrast into the prostate. There is no evidence of reflux of contrast in the ureters. Also there is unremarkable contrast filling of the urinary bladder. The focal narrowing of the prostatic urethra is concerning for fibrosis or cicatrisation from previous trauma given the healed/chronic pelvic fractures.
Figure 2. Lateral (left) and dorsoventral (right) radiographs acquired following a retrograde urethrogram. Both radiographs show the narrowed region of the prostatic urethra (indicated by the red arrow) and reveal the non-union fracture of the left acetabulum (highlighted by the red circle).
Diagnosis:
Urethral stricture and pelvic fractures
Plan:
We will attempt to use a balloon dilator to stretch the stricture, or we will consider using a urethral stent